|
|
||||||||||
|
|
 |
|
|||||||||
|
|
|
 |
|
||||||||
|
|
|
||||||||||
|
|
|
||||||||||
|
|
|
||||||||||
|
|
|
||||||||||
|
|
|
||||||||||
|
2011, Vol. 6 No. 1, Article 83
Umbilical Hernia with Abomasal-Umbilical Fistula in a Cow Calf Vandana Sangwan*1, Ashwani Kumar2, Kiranjeet Singh2 and Shashi Kant Mahajan2
1Department of Teaching Veterinary Clinical Complex 2Department of Veterinary Surgery and Radiology, College of Veterinary Science
College of Veterinary Science,
*Corresponding Author; e-mail address: [email protected]
ABSTRACT An unusual case of Umbilical hernia with umbilical-abomasal fistula at two sites in a two months old female calf was reported. Uneventful recovery was observed following successful surgical management of the ailment. KEY WORDS Umbilical hernia, abomasal fistula, calf, surgery. INTRODUCTION Umbilical hernia with entrapment of abomasum in the hernial ring in cow calves is not uncommon but its incarceration and necrosis resulting in formation of abomasal fistula is rare. Umbilical-abomasal fistula may be critical as there is continuous loss of digesta along with digestive secretions from an unusual site which may further alter the electrolyte and acid base status of the calf. The present report describes the successful surgical management of an umbilical hernia with an umbilical-abomasal fistula in a 2 month old female calf. CASE HISTORY AND CLINICAL SIGNS A two month old female cow calf was presented to the Teaching Veterinary Hospital with a swelling at the umbilical region and two red coloured masses protruding out of it from two sites (Fig. 1). Green coloured digesta was leaking out from these sites. History revealed presence of small umbilical swelling since one month which was gradually increasing in size. The swelling ruptured a day before presentation. Clinically, the calf was partially anorectic, thin, depressed and severely dehydrated. The umblical mass was big and no attempt to see the reducible character was made to avoid contamination to the peritoneal cavity. The pH of the green digesta leaking from the wound was noted to be acidic (pH 2) in nature. DIAGNOSIS AND TREATMENT
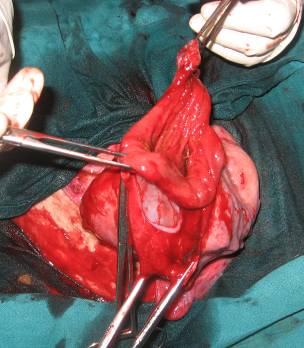
On the basis of history, clinical signs and pH of the contents, the case was diagnosed to be umbilical hernia with umbilical-abomasal fistula at two sites. Intravenous fluid therapy was started with Inj. NSS (0.9%). The animal was put in dorsal recumbency and prepared aseptically for surgery. Local anesthesia was given by infiltrating inj. lignocaine hcl 2% around the swelling. An elliptical skin incision was made to resect the infected tissue. A 12 cm long segment towards the pyloric end of abomasum (between body and pyloric end of abomasum) was found adhered to the hernial sac (Fig. 2). The other side of the abomasal wall was healthy. The abdominal cavity was packed with drapes to avoid contamination. The abomasum adhering to the hernial sac was carefully dissected out and a wedge shaped resection of the necrosed portion was done (Fig. 3). To avoid reducing the lumen size of the pyloric end the abomasum the abomasotomy wound was sutured perpendicular to the abomasal axis (Fig. 4) using a double layer of lambert suture pattern using Catgut No. 1-0. The sutured part of the abomasum was thoroughly flushed using normal saline solution and placed back into the abdomen. The hernial ring was closed by applying vest over pant pattern using silk No.2. Skin was closed using horizontal mattress sutures with silk No.2.
DISCUSSION
The pyloric part of the abomasum is usually herniated in umbilical hernia in cow calves but presence of umbilical-abomasal fistula is rare (Fubini and Ducharme 2004). Abomasal fistulas have also been reported to occur as a technique related complication of abomasopexy in cattle (Parker and Fubini 1987; Fubini and Ducharme 2004). From the history, the present case appeared to have an umbilical hernia with incarceration of abomasal wall which gradually developed into a fistula which is similar to findings by Fubini and Smith (1984). Since the present calf was on green fodder diet, the pressure of food in the pyloric part of abomasum might be responsible for its simultaneous rupture at two sites. Such rupture at two sites has not been reported in the literature. Umbilical-abomasal fistula has also been reported in calves from an umbilical infection invading the underlying tissue and eventually the abomasum (Newcomb and Mortom 1970) which was not apparent in this case.
REFERENCES
FIGURES Figure-1: Photograph showing swelling at the umbilical region and protrusion of red colored mass out of it from two sites
Figure-2: Photograph showing adhesions of a segment of pyloric part of abomasum to the hernial sac or skin
Figure-3: Photograph showing abomasotomy wound after resection of necrotic tissue
Figure-4: Photograph showing sutured abomasotomy wound
|
|
||||||||||
|
|
|||||||||||
|
|
|||||||||||
|
|
|||||||||||
|
|
|||||||||||
|
Copyright © Vet Scan 2005- All Right Reserved with
VetScan |
Home | e-Learning |Resources | Alumni | Forum | Picture blog | Disclaimer |
|
|||||||||
|
powered by eMedia Services |
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|