|


2011, Vol. 6 No. 2, Article 93
Dilated Cardiomyopathy in Dogs:
A Study for 3 Years (2006 To 2009)
K. Satish Kumar*, D. S. Tirumala Rao and P. Nagaraj
Department of Veterinary Clinical Medicine
College of Veterinary Science, Rajendranagar
Hyderabad – 500 030,
Andhra Pradesh, India
*Corresponding Author;
e-mail address: [email protected]
ABSTRACT
Out of 872 dog suspected for cardio-pulmonary disorders, 228 dogs were diagnosed for various cardiac abnormalities, of which 120 (52.63%) were confirmed as DCM, with a prevalence rate of 26%. Fifty (41 male and 09 female) medium to large breed dogs weighing 20-32 kg, aged between 08-14 years selected for detailed analysis were equally allotted to two groups for therapeutic trial with different treatment regimes. Elevated levels of Creatine Kinase MB and Lactate Dehydrogenase were the significant biochemical abnormalities. A significantly (P<0.05) increased LVEsD, LVEdD and EPSS with decreased IVSsD, IVSdD, LVPWs, LVPWd were associated with the left ventricular dimensions. Though alleviation of signs started from 3-5 days among both the groups, complete clinical recovery was noticed after 25 - 35 days in enalapril treated group and by day 50 in losartan potassium treated group.
KEY
WORDS
Dilated cardiomyopathy, diagnosis, therapy, dogs.
INTRODUCTION
Cardiomyopathies are recognized as common ailments in small animal clinical practice. Among cardiomyopathies, Dilated Cardiomyopathy (DCM) remains as an independent risk factor for the chronic morbidity and mortality (Thomas, 1987). DCM is characterized by impaired myocardial function (systolic +/- diastolic), ventricular dilatation and frequently, tachyarrhythmias. The etiology of the myocardial hypokinesis is seldom known in the individual case of DCM, although several theories concerning genetic, nutritional, metabolic, inflammatory, infection or drug or toxin induced myocardial diseases have been hypothecated (Kathryn, 2005). Breed specific predispositions has been observed in dogs. Doberman pinscher, Great Dane, German shepherd, Scottish deerhound and Irish wolfhound appear to be over represented. This article will discuss clinical presentation, diagnosis, screening and new trends in treatment for canine DCM.
MATERIALS AND METHODS
The present investigation was carried out at Teaching Veterinary Clinical Complex (TVCC), College of Veterinary Science, Hyderabad, Andhra Pradesh, India over a period of 3 years (2006-2009). Out of a total of 872 dogs of different breed, age and sex referred from various hospitals to Cardiology section with the manifestations suggestive of cardio-pulmonary disease, 228 were diagnosed for various cardiac abnormalities and out of which, 120 dogs based on echocardiographic findings were confirmed for DCM and of which 50 DCM dogs of medium to giant breeds weighing 20-32 kg, aged between 08-14 years selected for detailed analysis and were equally allotted to two groups for therapeutic trial with two different treatment regimes. Fifty DCM dogs selected for study comprised of 17 Doberman pincers, 12 German shepherd, 13 Labrador retriever, 06 Boxers and 2 Great Dane. Electrocardiography was performed on right lateral recumbancy using BPL Cardiart 1608 and whereas the radiographic evaluation was done on left lateral and ventro - dorsal exposures using Siemens X-ray unit. Blood samples were collected for complete blood count, serum biochemical profile and thyroid profile. Canine heart worm was detected by heartworm antigen test using Agen CHW® kit. Cardiac ultrasonography was performed using
Ixos vet ultrasound / Doppler machine supplied by Esoate Pie Medicals, Netherlands.
Following echocardiographic aspects were studied using a micro convex Array C5-2 R13 cardiac probe:
M-Mode Echocardiography
Transthoracic echocardiograms were obtained with the unsedated dogs on right lateral recumbancy. Access to the right side of the thorax was facilitated by use of a table with a special cut-out to allow the transducer to be directed upward towards the site of maximal cardiac pulsation as suggested by Allworth et al (1995). Transducer was located parasternally between right third and sixth intercostals between sternum and costochondral junction (Thomas et al., 1994).
M-Mode Measurements
M-mode recordings were taken at the high papillary level. Measurement of left ventricular dimension at end–diastole (LVEdD) and at end–systole (LVEsD) was made intraluminally from the trailing edge of the septal wall image to the leading edge of the ventricular free wall. End–diastolic and end–systolic measurements of the thickness of the Inter Ventricular Septum (IVSd, IVSs) and left Ventricular Posterior Wall (LVPWd, LVPWs) were made using trailing edge (Allworth et al 1995). Further, Ejection fraction (EF) and Fractional Shortening (FS) were also obtained.
End point septal separation (EPSS) was measured from the point of maximal cranial motion of the cranial mitral valve leaflet (E point) to the interventricular septum during the rapid–filling phase of diastole (Calvert and John, 1986). All the measurements were made in millimeters. Further, pulsed wave Doppler and colour flow Doppler studies were also attempted in order to assess the mitral valve insufficiency and regurgitation as per the technique suggested by Dominique and Marc-Andre (2008).
Treatment
The 50 medium to giant breed DCM patients weighing more than 20 kg were randomly divided into two groups viz., group I and II, with 25 in each, for therapeutic trial. Group I dogs were treated with oral enalapril @ 0.5 mg/kg and dogs of group II were treated with losartan potassium @ 25 mg/dog, BID for 30 days, followed by SID for 60-90 days. Spiranolactone @ 0.5 mg/kg was administered BID for 15 days to ascites / pedal edema dogs and SID for 15 days to the remaining dogs. Levo-carnitor @ 30 mg/kg, SID was administered for 90 days to all the 50 dogs of both the groups The data was statistically analyzed using paired t test.
RESULTS
Out of 872 dogs, 120 (52.63%) dogs (89 male, 31 female) were confirmed for DCM. with a highest prevalence rate of 25.82% in Doberman followed by German shepherd (21.20%), Labrador retriever (19.48%), Boxer (10.20%), Dalmatian (7.36%), Non-descript (7.28%), Pomeranian (7.00%) and Great Dane (1.66%).
General clinical manifestations included, decreased exercise tolerance, poor appetite, lethargy, generalized weakness and cough for more than a couple of weeks. Mild systolic murmurs with tachy-arrhythmias were detected on auscultation of cardiac area on left side of thorax between 3rd to 5th intercostals and mild crackles over lung area. Irregular seizures (09dogs), mild syncope (06dogs) and combined signs (05 dogs) were also reported during physical exertion. Physical examination revealed lethargy, ascites (08 dogs), pedal edema (12 dogs) with respiratory distress.
The mean haematological parameters of total erythrocyte count, haemoglobin, total leukocyte count and differential count were well within the normal range. The mean creatine kinase MB (71.8 ± 0.44 U/L) and lactate dehydrogenase (128.18 ± 1.84 U/L) levels were higher than the normal ranges of 24.26 ± 0.14 U/L and 72.45 ± 0.28 U/L respectively. Other serum biochemical parameters (total serum proteins, albumin, aspertate amino transferase and cholesterol) were with in the normal range. No abnormality was detected with the values of T3, T4 and TSH. Test for heartworm antigen was also negative.
Electrocardiographic abnormalities include increased R and P wave amplitude, ventricular premature complexes, ventricular tachycardia, deep Q wave, ST coving, wide and bizarre QRS complexes. Thoracic radiography revealed cardiomegaly with increased sternal contact in all the dogs and moderate pulmonary edema among 18/50 suggestive of left side heart failure (fig. 1). Whereas, abdominal radiograph in dogs with pendulous abdomen revealed ground glass appearance and loss of overall visceral detail, consistent with ascites. Abdominal ultrasonography also revealed anechoeic area in the abdominal cavity with floating viscera suggestive of fluid accumulation.
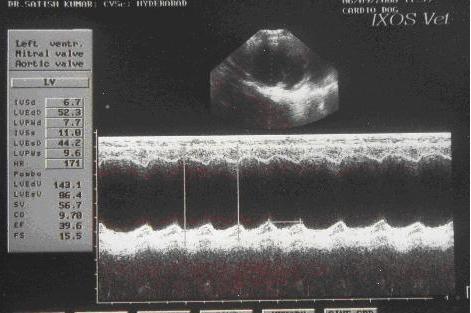
2-D echocardiograpy of DCM dogs revealed globose heart with dilated ventricles and/or atria on short axis view (fig.2). Whereas, m-mode echocardiography revealed thin interventricular septum (IVS), left ventricle posterior wall (LVPW) with increased internal diameter of the left ventricle both at diastole and systole (fig. 3). The left ventricle dimensions at end diastole (LVEdD) and systole (LVEsD) values of the DCM dogs of group I and II on day 0 (before treatment) were 57.17 ± 0.58 and 49.67 ± 0.57; 56.57 ± 0.87 and 49.59 ± 1.38 mm, respectively that were significantly increased (P<0.01) when compared to the mean values of healthy dogs (41.98 ± 0.39 and 34.55 ± 0.49 mm). These dimensions after therapy (by day 90) decreased significantly (P<0.05). The other dimensions viz., LVPWd, LVPWs, IVSd, IVSs and EPSS noted on day 0 were significantly (P<0.05) decreased and increased, respectively. Following therapy (on day 90) a non-significant increase in the dimensions of LVPWd, LVPWs, IVSd, IVSs with a non-significant decrease in EPSS was noticed. With respect to Ejection Fraction and Fractional Shortening, the values on day 0 were significantly (P<0.01) low when compared to healthy dogs. However, a significant (P<0.05) increase in these values were recorded following therapy (Table 1 and fig. 4).
Based on the echocardiographic, radiographic and electrocadiographic findings, the condition was diagnosed as dilated cardiomyopathy. All the dogs of both the groups started clinical improvement from day 3 to 5. The crackles and murmurs that had been auscultated were diminished in intensity, less frequent cough and the amount of ascitic fluid and pedal edema was noticed declining from day 5. Complete alleviation of clinical signs with absence of cough, ascites and pedal edema, improvement in physical activity and appetite was observed by day 35 and 50 in DCM dogs of groups I and II, respectively. However, the owners of the respective group dogs were advised to continue enalapril and losartan along with carnitor for 90 days. It was reported that all the dogs continued to improve and became much brighter and active over next 30 days except 1 GSD and 3 Dobermans (1 from group I and 3 from group II) died during the course of therapy. After therapy no appreciable changes in heart size on thoracic radiographs were noticed except absence of pulmonary edema. Similarly except absence of arrhythmias, no difference in ECG was detected. Whereas, left ventricular dimensions in both the groups improved by day 90 when compared to day 0, along with a significantly (P<0.05) different LVEdD and LVEsD values between the groups, that were treated using Angiotensin converting enzyme inhibitors (enalapril) and Angiotensin receptor blockers (losartan potassium), respectively (Table. 1).
DISCUSSION
DCM in dogs is more often diagnosed after the onset of CHF, but can be diagnosed well in advance by echocardiography, after detection of a cardiac gallop or murmur. DCM occurs in dogs of all ages, but the risk increases substantially with advanced age. The majority of dogs with DCM were more than 6 years of age (Kathryn, 2005). Signs of acute left side heart failure or life threatening arrhythmias are generally encountered in Dobermans and Boxers. Syncope and/or sudden death may be the first observed sign in these breed dogs with DCM. Other large breed dogs have lower possibility to syncope or to die suddenly. Ascites and / or pleural effusion are even more prevalent in other giant breed than Dobermans and Boxers. Weight loss and muscle wasting is common in some dogs with DCM. These findings are more severe in some dogs that have been symptomatic for several months. A regurgitant systolic murmur with a low-pitched protodiastolic gallop sound are frequent and important clinical finding. A gallop sound is evidence of severe ventricular impairment (Kathryn, 2005).
Electrocardiographic abnormalities particularly atrial fibrillation, ventricular premature complexes and ventricular tachycardia are common in DCM dogs. These arrhythmias may be present up to nine months prior to the development of echocardiographic evidence of this disease in certain breeds like Dobermans. In Boxers sudden death due to this cardiac complaint is less common when compared to Dobermans. Other ECG abnormalities include elevated R and P waves with deep Q wave and ST coving. However, abnormalities of cardiac conduction have been diagnosed in 38 % of dogs and changes in wave morphology have been recorded in 62 % of patients. Pulmonary edema is the most common finding on thoracic radiographs of dogs with symptomatic DCM, although signs of right side heart failure are reported to be common in giant breeds. Radiographic changes affecting the cardiac silhouette include left atrial enlargement alone, left atrial and left ventricle enlargement, right sided enlargement or generalized cardiomegaly (Allworth et al., 1995 and Kathryn, 2005).
Echocardiographic evaluation of left ventricle systolic performance reveals increased end-systolic and end-diastolic dimensions, dilatation of left atrium and decreased fractional shortening and ejection fraction in dogs with DCM. Significant (P < 0.01) increase was observed in cardiac dimensions in both the long and short axes and in end-diastolic and end-systolic volume. This was associated with the left ventricle assuming a more spherical shape. Both isovolemic and ejection phase indices were depressed by 50%. The end-systolic elastance was also depressed significantly in dilated congestive cardiomyopathy dogs (Shannon et al., 1991).
A strong male predisposition in the Great Dane suggests an X-linked mode of inheritance (Hammer et al., 1996 and Meurs et al., 2001). Dogs exhibiting the clinical signs of DCM do not always respond to conventional medical therapy of congestive heart failure. A complete cardiac evaluation, including echocardiography is essential in determining the exact cause and advocate correct treatment for DCM patients.
Angiotensin converting enzyme inhibitors are of more valuable in treating DCM dogs, as the dogs in the present report resulted in a sustained improvement in clinical signs for several weeks. In landmark veterinary studies of enalapril in NYHA phase III and IV heart disease (moderate to severe heart failure), due to mitral regurgitation (MR) and dilated cardiomyopathy (DCM), enalapril improved survival by >100% as well as reducing pulmonary edema and improving quality of life scores. Exercise capacity is also improved in dogs with experimental mitral insufficiency. Benazepril has likewise been shown to improve survival. Whereas, β-blockers (carvedilol) treatment did not result in significant changes in echocardiographic, neurohormonal activation, radiographic heart size, heart rate, or owner perceived quality-of-life over a 4-month treatment period, even though it was hypothecated that the drug improves echocardiographic and neurohormonal variables in dogs with DCM (Oyama et al., 2007). However, ACE-I have proven to provide additional benefits in human patients by blocking pathological remodelling, presumably slowing progression of heart disease and by normalizing serum electrolyte concentrations. Today, ACE-I represent the cornerstone in the chronic management of CHF. They are indicated in virtually all cases of systolic heart failure in which they are tolerated (Atkins, 2007). Losartan potassium was the first orally bioavailable, long-acting, nonpeptide Angiotensin receptor antagonist to be used in humans. The most frequent adverse reaction, as observed in a clinical trial of 2900 patients assessing the safety and tolerability of losartan-20 was dizziness, reported in 4.1% of patients taking losartan versus 1.3% of placebo recipients. Other adverse events (headache, upper respiratory tract infections, diarrhoea, fatigue and cough) occurred with similar frequencies in the losartan and placebo groups and thus were not considered drug related (Raquel and Mahtab, 2000). In the present study no such adverse reactions were found.
ACE inhibitors have been used extensively in heart failure, they induce systemic vasodilatation. They have also been shown to reduce ischemic events after myocardial infarction, although their mechanism of action on the coronary circulation is less understood. Nikolaidis et al., (2002) opined that the ACE inhibitor, enalapril improves transmural myocardial perfusion at rest and after chronotropic stress and restores impaired subendocardial coronary flow and vasodilator reserve in DCM. The effects of enalapril were bradykinin mediated and nitrous oxide dependent and were not recapitulated by losartan, that suggest beneficial effects of ACE inhibitors on the coronary circulation in DCM that are not shared by AT1 receptor antagonists. In the present study the dogs of group I that received ACE inhibitor (enalapril) have shown faster and complete clinical recovery with in a shorter period along with a significantly different left ventricle dimensions when compared to the dogs of group II that received AT1 receptor antagonist (losartan potassium).
CONCLUSION
From the present study it may be concluded that the dilated cardiomyopathy is a common cardiac disorder among medium to giant breed dogs weighing more than 20kg. Electrocardiographic, radiographic and cardiac enzymes evaluation is the diagnostic protocol but echocardiography is the most sensitive means of diagnosis. Angiotensin converting enzyme inhibitors is more efficacious when compared to Angiotensin receptor antagonists in improving the condition.
REFERENCES
-
Allworth, S. M., Church, D. B., Maddison, J. E., Einstein, R., Brennar, P., Anssein , N. A. and Mathews, R. 1995, Effect of enalapril in dogs with pacing induced heart failure. Am. J. Vet. Res. 56, 86-94.
-
Atkins, C. E. 2007, Angiotensin Converting-Enzyme Inhibitors and the Kidney Proceedings, World Small Animal Veterinary Association World Congress Proceedings.
-
Calvert, C. A. and John, B. 1986, Use of M-mode echocardiography in the diagnosis of congestive cardiomyopathy in Doberman pincers. J. Am. Vet. Med. Assoc. 189, 293-297.
-
Dominique, P. and Marc-Andre d’ Anjou. Atlas of Small animal Ultrasonography. I edn., Blackwell Publishing, Australia, 2008, pp. 780-824
-
Hammer, T. A., Venta, P. J. and Eyster, G. E. 1996, The genetic basis of dilated cardiomyopathy in Doberman pinschers. Anim. Gen. 27, 101-119.
-
Kathryn, M. M. 2005, Canine dilated cardiomyopathy – insights into diagnosis and mangement. Proceeding of the NAVC North American Veterinary Conference. Florida, 19-122.
-
Meurs, K. M., Miller, M. W. and Wright, N. A. 2001, Clinical features of dilated cardiomyopathy in Great Danes and results of a pedigree analysis: 17 cases (1990-2000). J. Am. Vet. Med. Assoc. 218, 729-732.
-
Nikolaidis, L. A., Doverspike, A., Huerbin, R., Hentosz, T. and Shannon, R. P. 2002, Angiotensin-converting enzyme inhibitors improve coronary flow reserve in dilated cardiomyopathy by a bradykinin-mediated, nitric oxide-dependent mechanism. Circulation. 105(23): 2785-2790.
-
Oyama, M. A., Sission, D. D., Prosek, R., Bulmar, B. J., Leuthy, M. W. and Fuentes, V. L. 2007, Carvedilol in dogs with dilated cardiomyopathy. J. Vet. Intern. Med. 21(6):1272- 1279.
-
Raquel, D. and Mahtab, J. 2000, Angiotensin II-Receptor Antagonists: An Overview: Losartan Potassium. Am. J. Health-System Pharm. 57(13): 4-18.
-
Shannon, R. P., Komamura, K., Stambler, B. S., Bigaud, M., Manders, W. T. and Vatner, S. F. 1991, Alterations in myocardial contractility in conscious dogs with dilated cardiomyopathy. Am. J. Physiol. Heart Circ. Physiol. 260, 1903-1911.
-
Thomas, P. W., Gaber, C. E., Jacobs, G. J., Kaplan, P. M., Lombard, C. W., Moise, N. S. and Moses, B. L. 1994, Recommendations for standards in transthoracic two-dimensional echocardiography in the dog and cat. Vet. Rad. Ultrasound 35, 173-178.
TABLES
Table 1:
Mean ± SE of Left Ventricle dimensions of DCM dogs
|
S. No.
|
Parameter
|
Apparently healthy dogs
|
Group –I
|
Group -II
|
|
BT(day0)
|
AT(day90)
|
BT(day0)
|
AT(day90)
|
|
1.
|
LVEdD (mm)
|
41.98 ± 0.39
|
57.17** ± 0.58
|
51.52* a ± 0.77
|
56.57** ± 0.87
|
52.09* b ± 0.89
|
|
2.
|
LVEsD (mm)
|
34.55 ± 0.49
|
49.67** ± 0.57
|
41.00* a ± 0.59
|
49.59** ± 1.38
|
45.60* b ± 0.51
|
|
3.
|
LVPWd (mm)
|
6.76 ± 0.22
|
5.98* ± 0.51
|
6.23 ±0.22
|
5.54* ± 0.2
|
6.12 ± 0.24
|
|
4.
|
LVPWs (mm)
|
9.27 ± 0.18
|
8.38* ± 0.18
|
8.52 ± 0.23
|
8.28* ± 0.31
|
8.54 ± 0.11
|
|
5.
|
IVSd (mm)
|
5.82 ± 0.23
|
5.32* ± 0.36
|
5.5 ± 0.25
|
5.25* ± 0.22
|
5.49 ± 0.2
|
|
6.
|
IVSs (mm)
|
6.97 ± 0.21
|
6.39* ± 0.27
|
6.54 ± 0.11
|
6.19* ± 0.22
|
6.38 ± 0.2
|
|
7.
|
EPSS (mm)
|
4.62 ± 0.16
|
9.04* ± 0.13
|
8.78 ± 6.2 a
|
8.89* ± 0.15
|
7.92 ± 0.21 b
|
|
8.
|
FS (%)
|
38.12 ± 0.16
|
23.18** ± 0.98
|
29.70* a ± 1.32
|
22.33** ± 0.72
|
26.99* b ± 1.38
|
|
9.
|
EF (%)
|
60.88 ± 1.24
|
34.34** ± 1.88
|
50.66 **a ± 1.76
|
31.10** ± 1.92
|
40.72 **b ± 1.98
|
Means bearing same superscripts do not differ significantly
* Significant at (P<0.05)
** Significant at (P<0.01
FIGURES
Figure 1. Skiagram showing cardiomegaly and pulmonary and pleural effusion
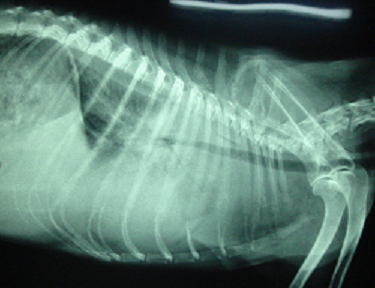
Figure 2. B-mode echocardiographic image showing dilated left ventricle (LV) and atrium (LA)

Figure 3. M-mode echocardiographic image showing increased left ventricle dimensions (day 0)
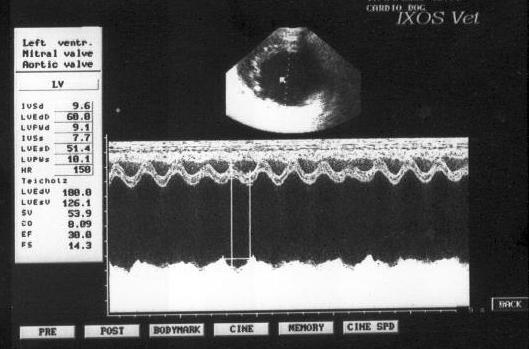
Figure 4. M-mode echocardiographic image showing left ventricle dimensions (day 90)
|
 |


